Excellence in Customized Scleral Lens Keratoconus Fitting
By Luciano Bastos, CLAO
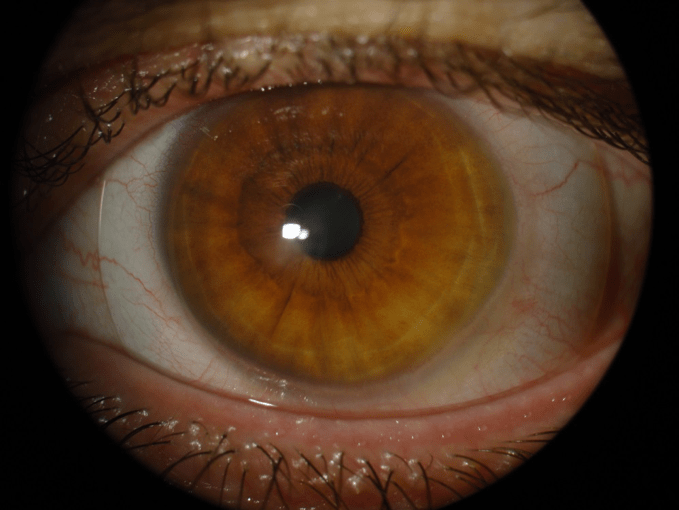
Patient male, 42 years old, he has binocular, stage IV keratoconus in OS. He also has stage III keratoconus at OD but is not as complex than at OS.
Back in 2007, we fitted him with Ultracone Advance, a specialty keratoconus RGP designed to allow fitting keratoconus conditions above 60 diopters base-curve. In the following years, we moved to an intralimbal version called Ultracone Extreme IL with a central base curve of 72 diopters. He was able to wear these special RGPs for 5 years but in 2013 we finally moved to a full scleral lens fitting. We fitted him with the SB Scleral lens I designed, manufactured by Ultralentes lab. Since 2013 he has worn his scleral lens all day long for about 16 to 18 hours without removal. Also, he has been refitted every two to three years.
In this article, we demonstrate how we customized the SB scleral lens at the OS where the case is very advanced. The images are from the last refit in July 2019.
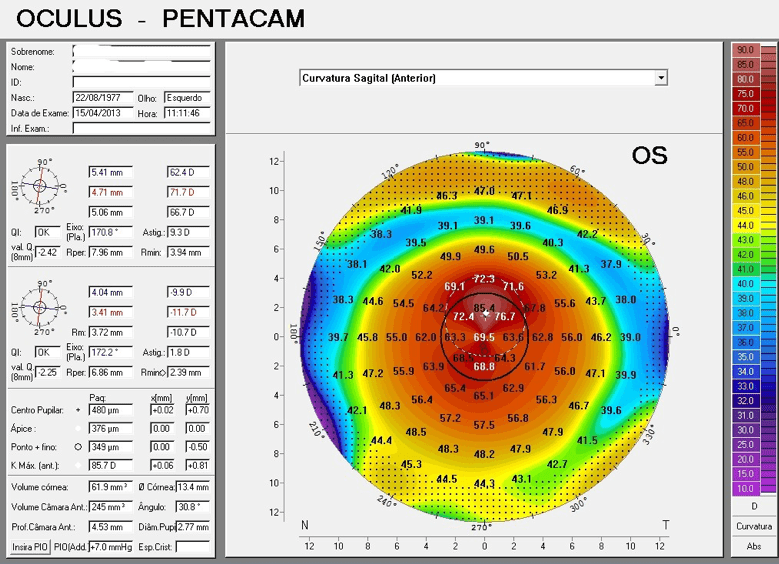
Fig. 02: Anterior Sagittal Curvature (Pentacam – 2013)
Images in figures 2 and 3 show the very advanced ectasia where RGP fitting is not feasible.
The SB Full Scleral lens trial set has two designs, one with a larger and single aspheric curve (called SB Full UF) and another with two base curves and two optical zones with different central base curve values (called SB Full UC). In this case, we fitted an SB Full UC which allow us to modify optical zone diameters and central and secondary base curve values in order to obtain the best alignment to the anterior eye profile in every quadrant. We first found the necessary SAG to overcome the entire cornea and limbus, then we needed to recalculate the SB Full lens parameters in order to decrease the height where necessary and still keep the SAG near the original value.
It is important to have some experience doing this but if you do not try you will not experiment and learn. Using software facilitates the analysis but what is crucial is a careful observation of the scleral lens profile in the eye using both biomicroscopy and tomographic images if available by Pentacam or OCT.

Fig, 03: Anterior eye OS profile.
Management of the Case
The SB Full scleral lens set offers a wide range of options of posterior, central base curve values which have a secondary base curve and the haptic, landing scleral zone. The goal, in this case, was to combine the best arrangement of the posterior base curves and its respective optical zone diameters in a way to provide the best possible alignment to the cornea and limbus, avoiding touch or an excessive vault. Figure 4 shows the excessive vault found with the trial lens and figure 5 shows the better alignment obtained after customizing the equation.
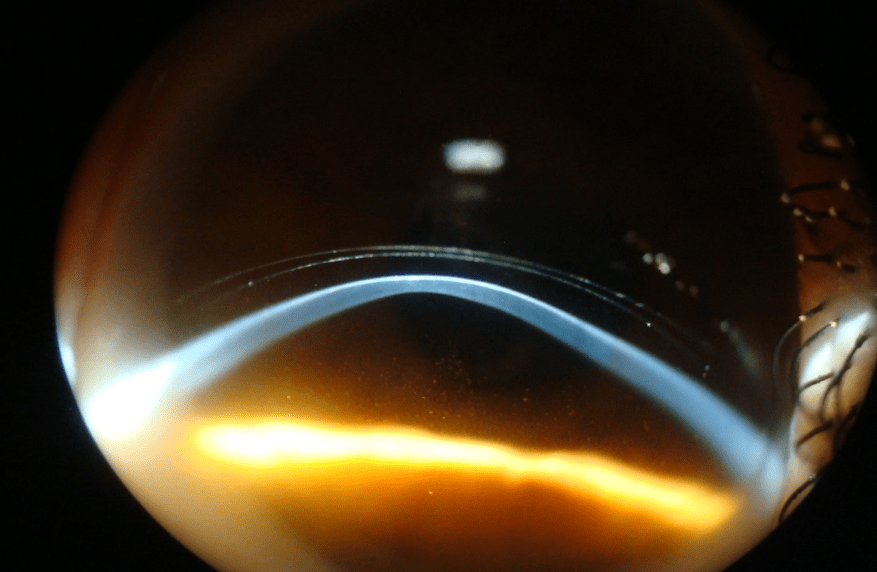
Fig.04: The scleral trial lens shows an excessive vault.
SAG 6.365
Material: Optimum Extreme Dk 125
In keratoconus cases with a profile that shows a central elevation at the apex we just increased the central posterior base curve radius but decreased the central optical zone, we flatten the secondary base curve radius so it will decrease the overall SAG and increase the secondary base curve diameter. These rightful rearrangements and the combination of equation variables which altered its radius and optical zone diameters helped to achieve a better alignment at the entire cornea and limbus as you can see in figure 5.
SB Full Scleral Lens After Customization
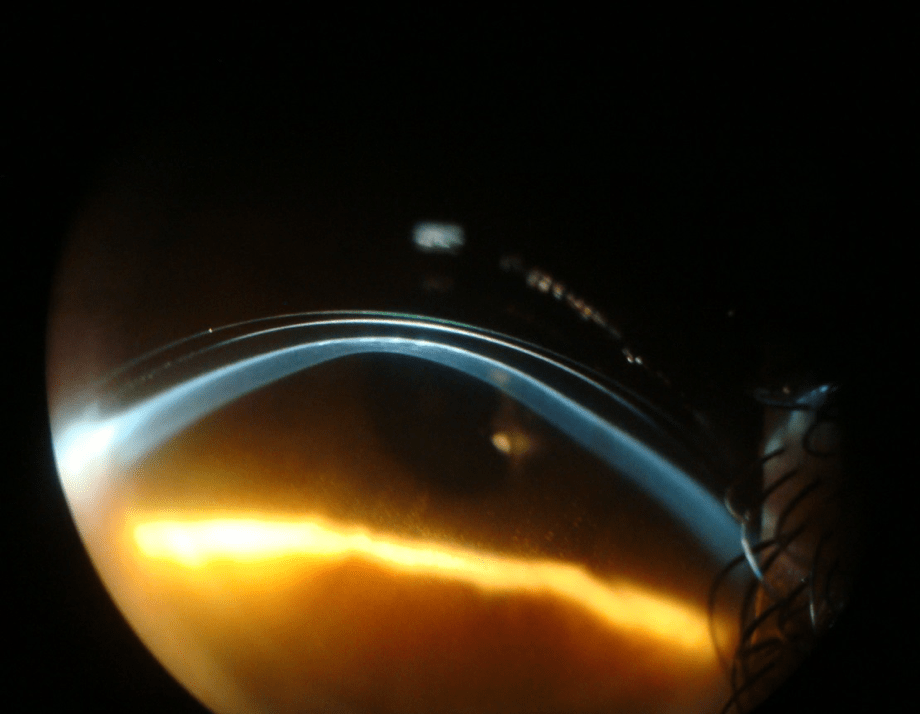
Fig.05: The customized SB Full scleral lens with optimization.
SAG 6.100
Material: Optimum Extreme Dk 125
It is interesting to note that scleral lens fitting often gives the practitioners an opportunity to improve the fitting with the next lens. Although both the specialist and patient may be satisfied with the result achieved it is always possible to improve the design to a better alignment at the next refit. Careful examination of the case, including documentation and images, will help, especially if it is a stationary case. The fact that the scleral lens is more forgivable, offers a wider range of options which can be experimented. These modifications require knowledge of the scleral lens design and which parameters can and should be changed. It is an equation where every variable you modify will ultimately result in a different SAG and profile pattern.
Conclusion
Scleral lens customization depends much on the amount of information the manufacturer provides the practitioners in respect of the design and the variables that may be changed.
If the manufacturer offers only a specific range of combination of parameters that cannot be changed you may not succeed in terms of a highly customized fit.
There are two main customizations that are necessary in scleral lens fitting, the first is the one explained in this article in order to achieve the best possible alignment and vault over the cornea and the limbus. The other is to accommodate the haptic when there is different angle at the scleral zones. It is quite common to see eyes where the sclera has a flatter angle in one or two positions, especially horizontal and a closed angle at the vertical position.
It helps if the lab provides the practitioner with the option to flatten or steepen the haptic, landing zone where it is necessary. Still, it also helps if the lab is able to apply specific modifications to avoid scleral obstacles like pinguecula by notching the lens of overcoming it with a specific posterior elevation at the haptic where the obstacle is localized.
It is of utmost importance to the practitioner to count on professional help from a lab manufacturer technician to show what variables can be altered and how they will impact on the final lens design. Also, it is crucial that the practitioner produces images from slit lamp photography as shown in figures 4 and 5. Another option would be the Pentacam Scheimpflug (Oculus Optikgeräte GmbH) images with the scleral lens or an OCT image covering the entire cornea and beyond the limbus.
Every change or combination of the scleral lens base curves, optical zone diameters and overall diameter will inevitably induce changes in SAG. It is also possible to obtain similar SAG values with a combination of these variables. There is a long learning curve in order to understand the impact of every combination of two or more variables. You need to use imagination and a starting point to initiate the changes and then use the contact lens design software to simulate these changes and observe the resulting SAG and how the finished design will impact the fitting.
The final evaluation will be when you see the patient after one or more hours after lens insertion. This will give enough time to the excess for fluid to get out so the SAG will be more realistic.
1. Customized Scleral Fit in a Case of Keratoconus – Contact Lens Spectrum, Volume: 28, Issue: September 2013, page(s): 30 – 37
2. Bastos L. ONLINE PHOTO DIAGNOSIS – Refitting a Corneal GP Lens Over a Scar December 1, 2018 –
Thank you to Luciano Bastos CLAO for contributing to Global Insight.
Luciano Bastos is the director and clinical instructor of specialty contact lenses at the Instituto de Olhos Dr. Saul Bastos (IOSB) and is the director and specialty lens consultant of Ultralentes, a small laboratory specializing in GP and scleral lens designs in Porto Alegre, RS, Brazil.